On being sane in insane places
Does a study from 1973 still hold lessons for us in 2026?
In the late 1980s I became enthralled with Professor David Rosenhan’s landmark study, “On Being Sane in Insane Places”. Even 52 years after it was published, (and even with the recent exposure of procedural flaws and questionable practices) it remains a touchstone in the critique of psychiatric diagnosis and the pervasive impact of institutional care – on patients and staff.
In summary, between 1969 and 1972, Rosenhan arranged for “normal” people or pseudo-patients, to feign symptoms in order to be admitted to 12 psychiatric institutions across five states in America.
All of the pseudo-patients were diagnosed and admitted with a mental illness (mainly schizophrenia). They remained in hospital for between 7 and 52 days before discharge. While none were identified by staff as “faking it”, a number of “real” patients voiced suspicions that the “pseudo-patients” were not actually ill; they thought they might have been journalists of professors checking up on the hospital.
As you can imagine there was an uproar from the psychiatric community when the initial results were shared. So Rosenhan conducted a second trial, this time advising a renowned psychiatric hospital that one or more pseudo-patients would attempt to gain admission during a specified period. As a result, of 193 patients, hospital staff identified 41 as potential impostors and a further 42 as suspect.
In reality, Rosenhan had not sent any pseudo-patients at all.
He argued that this further highlighted the unreliability and subjectivity of psychiatric diagnoses. It demonstrated how expectation and suspicion could lead to false positives, with staff mistakenly identifying genuine patients as fakes.
Rosenhan argued that the culture, context and expectations within psychiatric institutions significantly shaped how staff viewed their work and perceived patients. The study revealed subjective and sometimes arbitraryconstituents of psychiatric diagnosis. More critically it highlighted how closed institutional cultures and preconceptions impacted upon staff behaviour[s], practice and decision-making processes.
The study underscored how culture, context, expectations, and institutional culture can shape and sometimes distort perceptions of people and their roles – including staff. Patient experiences within such environments werecommonly marked by depersonalisation, powerlessness, and always a sense of being misunderstood / not being heard.
The report was published in 1973 – the same year that homosexuality, until then still considered a diagnosable and treatable mental illness, was removed from the DSM II.
This is a view strongly endorsed in 2018 He Ara Oranga[2] (the report of the 2018 Ministerial review into mental health and addiction) when arriving at two conclusions.
1) “New Zealand’s mental health and addiction problems cannot be fixed by government alone, nor by the health system.”
2) “We can’t medicate or treat our way out of the epidemic of mental distress and addiction...”
I have never regarded these conclusions as suggesting that there is no place for medical treatment in response to assessment and diagnosis. Instead, this about recognising that the diversity of challenges to people’s mental and emotional health in 2026 require a similar diversity of responses. The overarching goal of good mental health is sustainable communities; such communities have never been more diverse - and nuanced. Recognition of the importance of social determinants of mental health is not a trend in vogue; it is perspective that can no longer be marginalised by purely evidence-based approaches to healthcare.
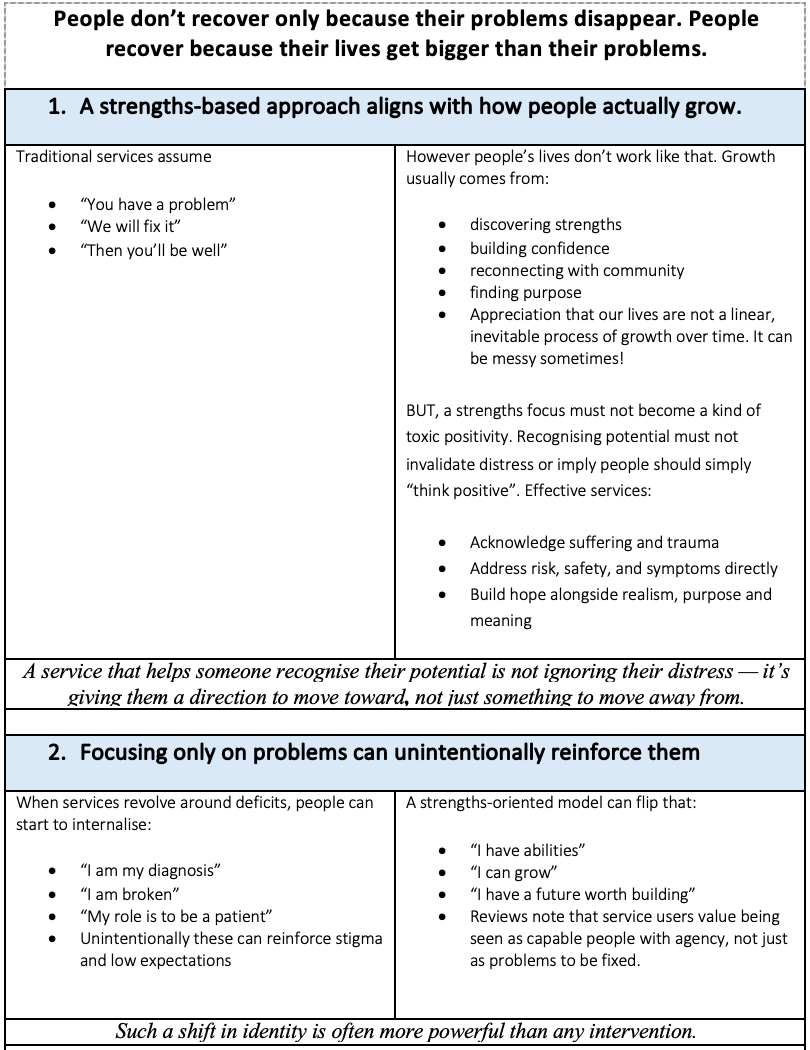
When services emphasise strengths, agency, and opportunity, people do tend to do better. Aways, this will work best when combined with support for distress, not instead of it.
[1] This conclusion very much replicates Franco Basaglia’s assertion that institutions are bad for people – harmful to patients and corrupting of the role of staff. (Staff too are subjected to the same institutionalising process as patients. They were infused into roles that focused on custody, rather than therapeutic relationships. Also, hospital life permeated a mood of exhaustion and malaise – that infected the wellbeing of both patients and staff.
[2] https://mentalhealth.inquiry.govt.nz/inquiry-report/he-ara-oranga page10
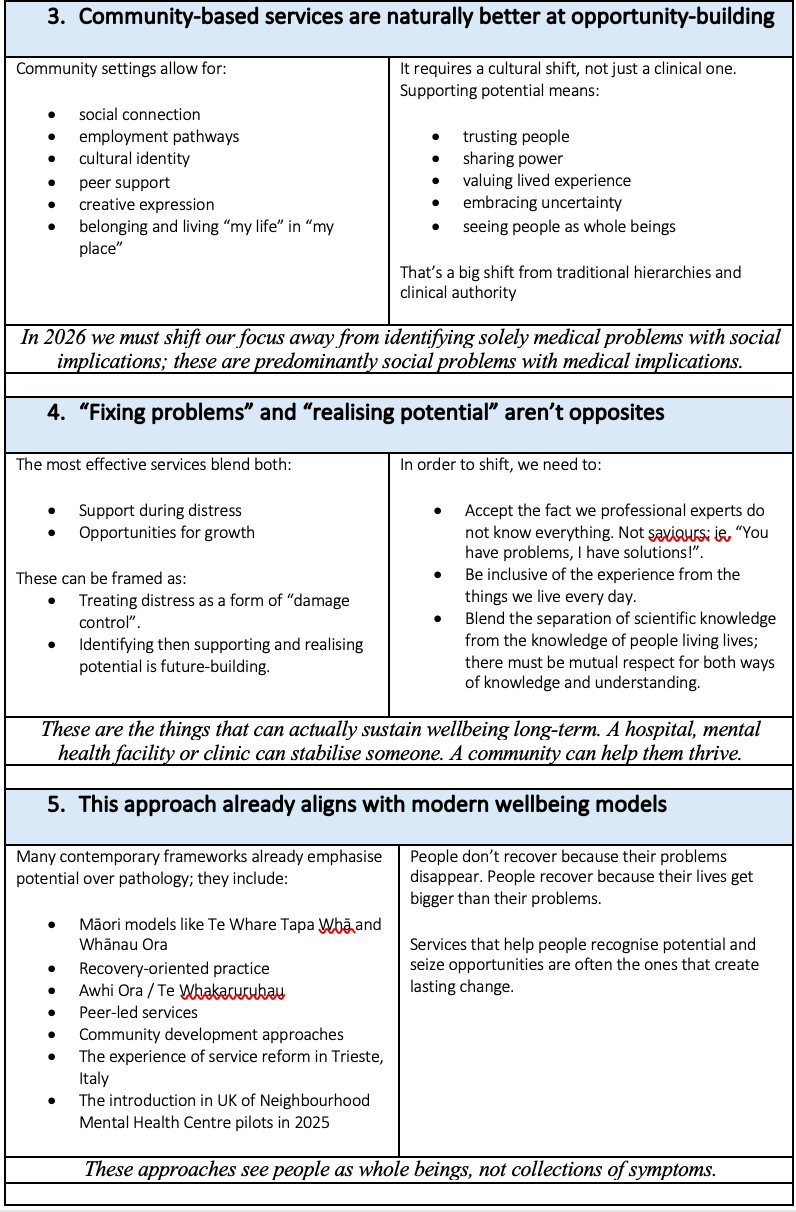
On Being Sane in Insane Places” was more than a just critique of psychiatric diagnosis within a rigidly institutional system. It is a call to reimagine mental health care and support as a fundamentally human endeavour. In 2026, the argument for community-based and community-led service development has become now both evidence-informed and ethically compelling. It is still resisted…
We can still learn much from Rosenhan’s theatrical expose of institutional psychiatry should remain a valid influence in how we prioritise, develop, then embrace contemporary community-based approaches. These must prioritise human rights, dignity, participation, social determinants, partnerships and social integration…
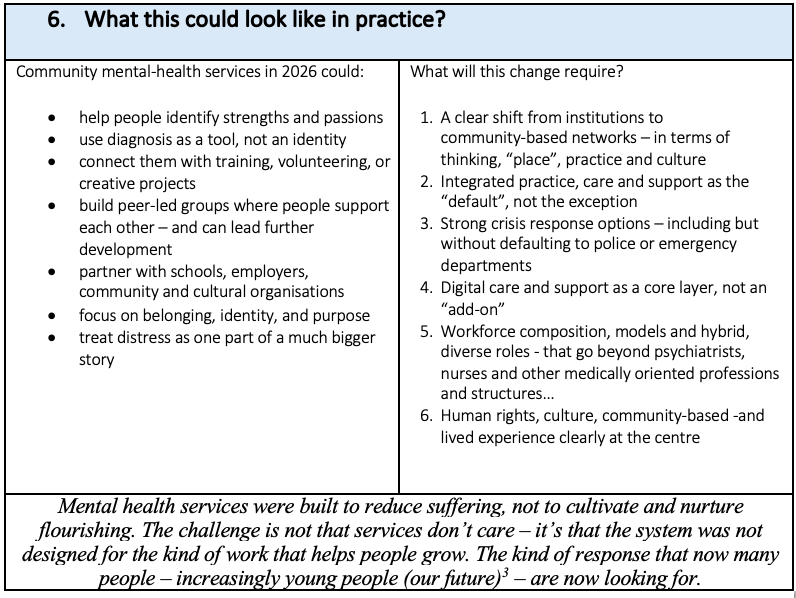
Now, more than ever before, we need mental health services (supported by contracting systems that serve and support human outcomes not outputs and compliance) that serve, are responsive and are relevant to the diverse needs of people and communities.
[1] Last year, a number of articles in The Times (UK) raised concerns about the 1000s of young people being abandoned to the welfare system, lost in addiction, isolation and/or despair. (Sickness benefits now cost more than the defence and police budgets combined).
The rise (250 people per day ) had been greatest for under 25s, who, “…feel dispossessed, they feel alienated because they are at the bottom of the pile”. ‘Mental health’ is the biggest reason for claims. “…people are experiencing real distress, whose causes may be debt, employment, housing, relationships, even their wider health – but the state can only respond by medicalising it as a mental health problem”.
God forbid that this should be a predictor of our future in Aotearoa New Zealand. For how many young people is this already their reality after leaving school?